| Authors |
Halperin RO, Sesso HD, Ma J, Buring JE, Stampfer MJ, Gaziano JM. |
|
| Title |
Dyslipidemia and the risk of incident hypertension in men |
|
| Full source | Hypertension. 2006 Jan;47(1):45-50 | |
|
|
Per scorrere le diapositive |
|
|
||
| Abstract |
Evidence
suggests that hypertension may share a similar pathophysiology with cardiovascular
disease (CVD). Thus, dyslipidemia, a strong predictor of CVD, may also
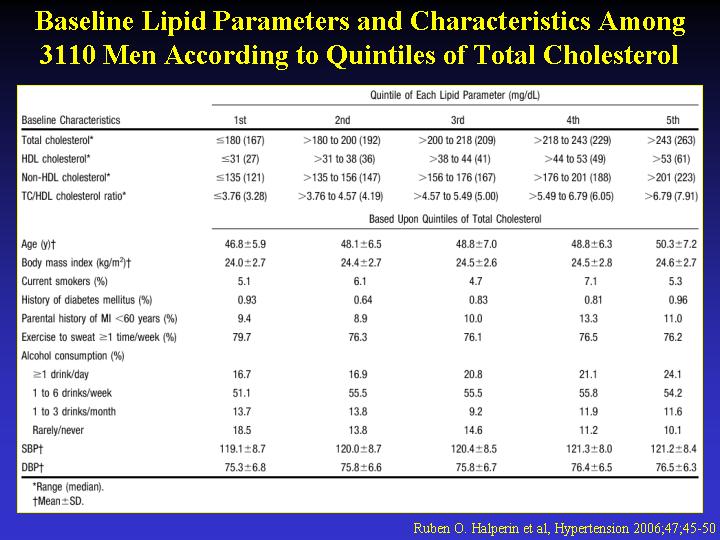
predict incident hypertension. We analyzed 3110 men free of hypertension,
CVD, and cancer from the Physicians' Health Study, who provided baseline
blood samples from which we measured total cholesterol (TC) and HDL cholesterol
(HDL-C), and calculated non-HDL-C and the TC/HDL-C ratio. We categorized
each lipid parameter into quintiles and considered National Cholesterol
Education Project clinical cut points. Other risk factor information was
provided from self-reports on the baseline questionnaire. Incident hypertension
was defined as either the initiation of antihypertensive treatment, self-reported
systolic blood pressure > or =140 mm Hg, or diastolic blood pressure
> or =90 mm Hg. Over a mean follow-up of 14.1 years, 1019 men developed
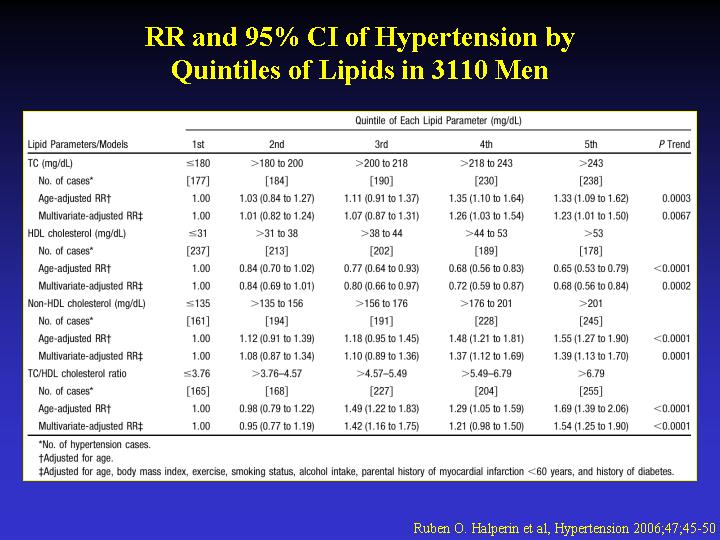
hypertension. In Cox proportional hazards models adjusted for lifestyle
and clinical risk factors, men in the highest quintile of TC, non-HDL-C,
and TC/HDL-C ratio had increased risks of developing hypertension of 23%,
39%, and 54%, respectively, compared with participants in the lowest quintile.
Furthermore, men in the highest quintile of HDL-C had a 32% decreased
risk of developing hypertension compared with those in the lowest quintile.
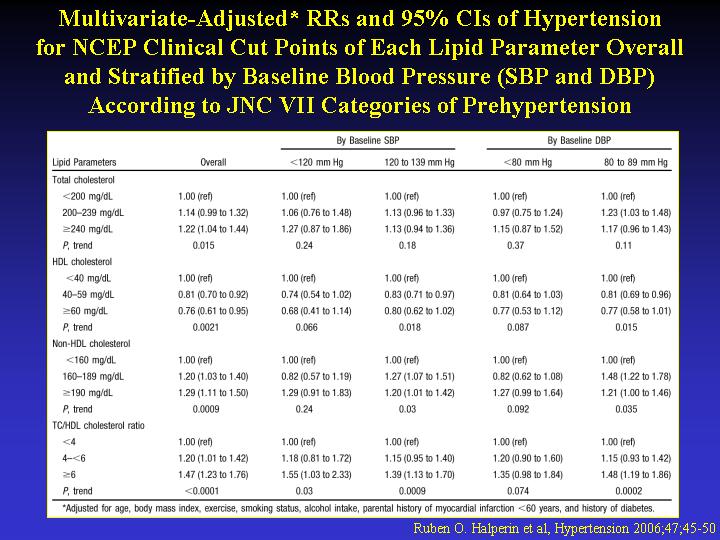
Models using National Cholesterol Education Project cut points demonstrated
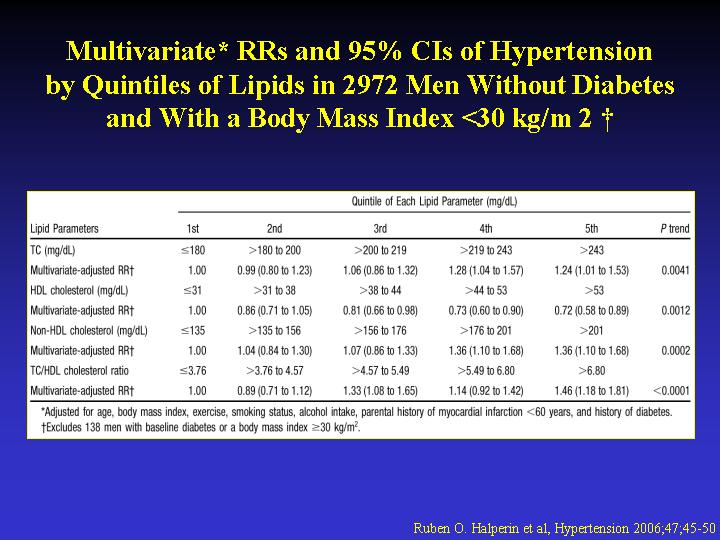
similar associations with hypertension. Models excluding men with diabetes
and obesity maintained an independent association between baseline lipids
and hypertension. These prospective cohort data suggest that dyslipidemias
may lead to the subsequent development of hypertension. Thus, plasma lipids
may be useful in the identification of men at risk for hypertension.
|
|