|
Aspirina
e prevenzione cardiovascolare: differenze tra uomini e donne
Aspirin for the
primary prevention of cardiovascular events in women and men: a sex-specific
meta-analysis of randomized controlled trials
Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL.
JAMA 2006;295:306-13
Abstract:
CONTEXT: Aspirin therapy reduces the risk of cardiovascular
disease in adults who are at increased risk. However, it is unclear if
women derive the same benefit as men.
OBJECTIVE:
To determine if the benefits and risks of aspirin treatment in the primary
prevention of cardiovascular disease vary by sex.
DATA SOURCES AND STUDY SELECTION: MEDLINE and the Cochrane Central Register
of Controlled Trials databases (1966 to March 2005), bibliographies of
retrieved trials, and reports presented at major scientific meetings.
Eligible studies were prospective, randomized controlled trials of aspirin
therapy in participants without cardiovascular disease that reported data
on myocardial infarction (MI), stroke, and cardiovascular mortality. Six
trials with a total of 95 456 individuals were identified; 3 trials included
only men, 1 included only women, and 2 included both sexes.
DATA EXTRACTION: Studies were reviewed to determine the number of patients
randomized, mean duration of follow-up, and end points (a composite of
cardiovascular events [nonfatal MI, nonfatal stroke, and cardiovascular
mortality], each of these individual components separately, and major
bleeding).
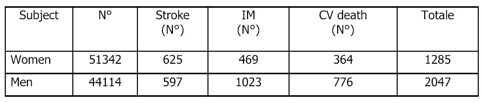
DATA SYNTHESIS: Among 51,342 women, there were 1285 major cardiovascular
events: 625 strokes, 469 MIs, and 364 cardiovascular deaths. Aspirin therapy
was associated with a significant 12% reduction in cardiovascular events
(odds ratio [OR], 0.88; 95% confidence interval [CI], 0.79-0.99; P = .03)
and a 17% reduction in stroke (OR, 0.83; 95% CI, 0.70-0.97; P = .02),
which was a reflection of reduced rates of ischemic stroke (OR, 0.76;
95% CI, 0.63-0.93; P = .008). There was no significant effect on MI or
cardiovascular mortality. Among 44,114 men, there were 2047 major cardiovascular
events: 597 strokes, 1023 MIs, and 776 cardiovascular deaths. Aspirin
therapy was associated with a significant 14% reduction in cardiovascular
events (OR, 0.86; 95% CI, 0.78-0.94; P = .01) and a 32% reduction in MI
(OR, 0.68; 95% CI, 0.54-0.86; P = .001). There was no significant effect
on stroke or cardiovascular mortality. Aspirin treatment increased the
risk of bleeding in women (OR, 1.68; 95% CI, 1.13-2.52; P = .01) and in
men (OR, 1.72; 95% CI, 1.35-2.20; P<.001).
CONCLUSIONS: For women and men, aspirin therapy reduced the risk of a
composite of cardiovascular events due to its effect on reducing the risk
of ischemic stroke in women and MI in men. Aspirin significantly increased
the risk of bleeding to a similar degree among women and men.
Commento:
Una meta-analisi
che ha coinvolto più di 50.000 donne e più di 40.000 uomini,
arruolati in 6 trials prospettici randomizzati, indica che una terapia
con aspirina a basso dosaggio è associata ad una riduzione significativa
di eventi cardiovascolari sia negli uomini che nelle donne, in prevenzione
primaria. Nello specifico diminuisce il rischio di ictus nelle donne e
di infarto del miocardio (IM) negli uomini.
Nelle donne la riduzione
di eventi cardiovascolari è del 12% ([OR] 0,88; 95% [IC] 0,79-0,99;
P=0,03) e del 17% quella di ictus ([OR] 0,83; 95% [IC] 0,70-0,97; P=0,02),
in termini soprattutto di ictus ischemico ([OR] 0,76; 95% [IC] 0, 63-0,93;
P=0,008). Nel gruppo degli uomini la riduzione di eventi cardiovascolari
è del 14% ([OR] 0,86; 95% [IC] 0,78-0,94; P=0,01) e del 32% quella
di IM ([OR] 0,68; 95% [IC] 0,54-0,86; P=0,001). La terapia con aspirina
aumenta però il rischio di sanguinamento ed emorragie in entrambe
i gruppi ([OR] 1,68; 95% [IC] 1,13-2,52; P=0,01 nelle donne; [OR] 1,72;
95% [IC] 1,35-2,20; P<0,001 negli uomini).


Questo studio, tuttavia
presenta delle importanti limitazioni; prima fra tutte il fatto di essere
una meta-analisi, quindi un'analisi retrospettiva che in quanto tale rimane
soggetta ai possibili limiti metodologici degli studi inclusi. Inoltre
va considerato che parametri fondamentali come la dose dell'aspirina,
la durata del trattamento e del follow up dei soggetti non risultano uniformi
fra tutti i trials considerati.
Ci sono poi varie possibilità per spiegare il diverso effetto cardioprotettivo
dell'aspirina sugli uomini e sulle donne; primo, è noto il diverso
metabolismo dell'aspirina nei due sessi. Numerosi studi hanno infatti
suggerito un ridotto effetto farmacologico dell'aspirina nelle donne,
rispetto agli uomini. Secondo, l'incidenza di ictus e di IM è differente:
le donne vanno incontro più facilmente ad ictus, gli uomini invece
ad infarto del miocardio. Terzo, la resistenza alle basse dosi di aspirina
tende ad essere più comune tra le donne che tra gli uomini.
Sulla base di dati clinici e di laboratorio, le attuali linee-guida raccomandano
una dose di aspirina compresa tra 75 mg/die e 12 mg/die in prevenzione
primaria.
Alberico
L. Catapano e Alessandra Bertelli, Dipartimento di Scienze Farmacologiche,
Università degli Studi di Milano
|
