
| Author | Jan-Christian Reil and Michael Böhm. |
| Title | BEAUTIFUL results—the slower, the better? |
| Full source | Lancet 2008;372:779-780 |
| Text |
In today's Lancet, Kim Fox and colleagues report the BEAUTIFUL results (from the trial called morBidity-mortality EvAlUaTion of the If inhibitor ivabradine in patients with coronary artery disease and left-ventricULar dysfunction).1If channels, in the sinoatrial node, are responsible for an inwardly directed current. This current has the noteworthy property of being activated by hyperpolarisation. Therefore the channel is activated during the resting potential stage and accelerates diastolic depolarisation of the sinus node and thus its pacemaker function. Because of this strange behaviour it was named funny current (I for current, f for funny).2 The BEAUTIFUL investigators studied patients with coronary artery disease, documented by previous angiography, myocardial infarction, and percutaneous or surgical revascularisation, and who also had left-ventricular dysfunction. Also reported is a subanalysis, which investigated the effect of heart rate on the primary composite of cardiovascular death, hospitalisation for acute myocardial infarction, and new onset or worsening of heart failure.3 BEAUTIFUL addresses the potentially important clinical and pathophysiological relevance of heart-rate reduction. Previous studies showed the effect of heart rate on outcome in the general population4 or in patients with hypertension,5 coronary heart disease,6 myocardial infarction,7 and heart failure.8 Data have largely been generated from epidemiological studies, and have led to the conclusion that heart rate might be a general denominator for pathophysiological mechanisms involved in cardiovascular complications.9,10 High heart rate is associated with important comorbidities in high-risk patients, such as those with microalbuminuria.11 Increased risk has been observed at rather low heart rates of 70–80 per min.4–11 Many pathophysiological studies identified potential mechanisms involved in the development of atherosclerosis, ventricular remodelling, and chronic heart failure, as well as comorbidities associated with these conditions (figure). The crucial remaining question is whether heart-rate reduction by drugs can reverse cardiovascular abnormalities—an epidemiologically lower resting heart rate might be associated with higher levels of physical exercise, less obesity, fewer comorbidities, and thus lower global cardiovascular risk that is not merely related to heart rate. 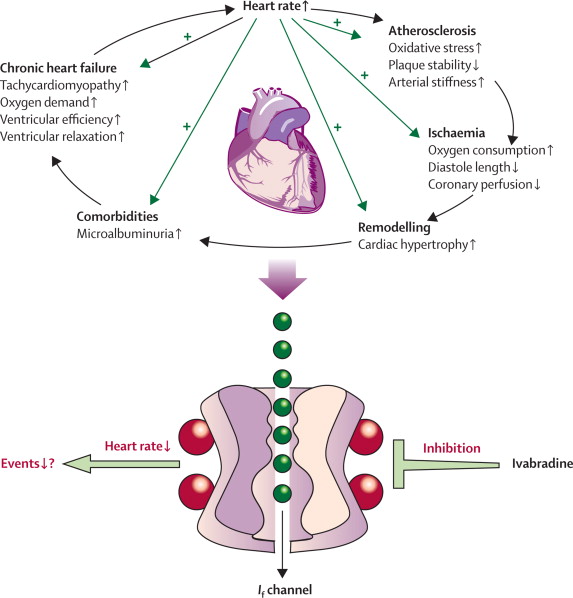
Potential
role of heart rate in cardiovascular pathology Clinical investigations into heart-rate reduction have been rendered possible by the development and clinical introduction of If-channel inhibitors such as ivabradine.12 Ivabradine has antianginal effects even when compared with a ß blocker,13 and angina is an approved indication for its use. In an atherosclerosis model, ivabradine reduced plaque load by 60–70%, when heart rate was reduced by 15%.14 Heart-rate reduction by ß blockers might be one beneficial mechanism achieved after myocardial infarction15 and in heart failure.16 Therefore heart-rate reduction beyond ß blockade by drugs appeared promising. The BEAUTIFUL investigators have added substantially to current knowledge by doing a well-designed and adequately powered controlled trial with relevant endpoints in patients, most of whom were pretreated with a ß blocker. The BEAUTIFUL subanalysis is in line with previous epidemiological investigations, in that it shows that the increase in cardiovascular endpoints happens at between 70 and 80 beats per min. BEAUTIFUL evaluated the effect of slowing heart rate with ivabradine in patients with established cardiovascular disease who were in sinus rhythm with a heart rate above 60 per min. The analysis was subdivided into a group of patients with heart rate above 70 per min and a group with heart rate below 70 per min. In the former group, there was a significant reduction of endpoints related to coronary heart disease, such as hospitalisation for myocardial infarction, unstable angina, and coronary revascularisations. In the latter group no such effects were seen. Neither of the groups showed change in all-cause mortality, cardiovascular death, or the other primary endpoints. These findings are in line with previous investigations, which have shown that ivabradine works beneficially on ischaemia-related symptoms.13 The baseline heart rate of the study population was around 70 per min with ß blockers, which seems rather low, and reasonable in patients with coronary artery disease. With an absolute reduction of 6 beats per min, by administration of ivabradine in addition to ß blockers, no additive beneficial effects were observed. More information about patients with higher heart rates (eg, above 80 per min), would be useful. 87% of patients received ivabradine in addition to ß-blocker therapy. Few patients were symptomatic and only 5% had to discontinue therapy because of bradycardia. Visual symptoms, including phosphenes, were unexpectedly rare (0·5%). BEAUTIFUL provides a large safety database for ivabradine in patients with significant cardiovascular disease at a heart rate in sinus rhythm above 60 per min. Most patients were taking ß blockers during the investigation. Although there was no significant difference whether patients were on (hazard ratio 1·00) or off (1·04) ß blockers, it would be useful to directly compare ivabradine with a ß blocker, to assess similarity of benefits and relative tolerability. Currently, however, such a trial might be ethically challenging to set up. Our knowledge of ivabradine will hopefully be enhanced by the Systolic Heart failure treatment with the If-inhibitor ivabradine Trial (SHIFT), which is studying a typical heart failure population. Further trials and subgroup analyses of BEAUTIFUL and SHIFT are needed to establish which patients benefit significantly from compounds, such as ivabradine, that target the sinus node. The BEAUTIFUL study has valuable lessons for clinical practice and illustrates the importance of individual decision-making. It remains to be seen whether or not the concept of the slower the better holds true. J-CR declares that he has no conflict of interest. MB has received research support from Servier. J-CR and MB are supported by the Deutsche Forschungsgemeinschaft (KFO 196). References
|