| Author | Elisabeth Mahla, Mark J. Antonino, Udaya S. Tantry, Paul A. Gurbel. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Title | Point-of-Care Platelet Function Analysis: Ready for Prime Time? | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Full source | J Am Coll Cardiol 2009;53:857-859 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Text |
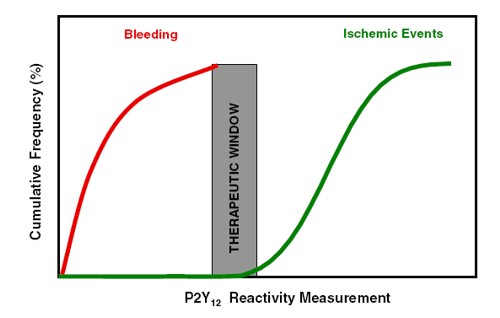
Dual antiplatelet therapy is effective in preventing ischemic complications after acute coronary syndromes and stenting. However, recurrent ischemic events and bleeding remain important concerns. Current practice guidelines advocate a "one-size-fits-all" antiplatelet strategy based on clinical trials that have largely avoided measurements of platelet function in the individual patient ( 1). Therefore, two burning unanswered questions remain: 1) is recurrent ischemic event occurrence primarily explained by high on-treatment platelet reactivity; and 2) is bleeding primarily explained by low platelet reactivity? The correct answers to these questions are crucial for the successful development of new antithrombotic strategies designed to improve patient outcomes. The unpredictable response to clopidogrel and the presence of high on-treatment platelet reactivity to adenosine diphosphate (ADP) in selected patients has been repeatedly shown by multiple methods that assess P2Y12 function, including light transmittance aggregometry (LTA), point-of-care whole-blood analysis of aggregation to fibrinogen coated beads, whole-blood flow cytometry to assess intracellular signaling and the expression of activation-dependent receptors, and thrombelastography (2,3). Poor responsiveness to clopidogrel was first linked to ischemic risk after stenting in patients with ST-segment elevation myocardial infarction in 2003. In a small study, Matetzky et al. ( 4) found that patients who showed the lowest quartile of platelet inhibition had a 40% probability for a recurrent cardiovascular event within 6 months. In the same year, Barragan et al. ( 5) reported an association between the platelet reactivity index measured by vasodilator-stimulated phosphoprotein (VASP) phosphorylation and the occurrence of stent thrombosis. In 2005 we reported an association between on-treatment ADP-induced platelet aggregation measured by LTA, 6-month post-stenting ischemic events, and stent thrombosis (6,7). Given the variability in baseline (i.e., pre-clopidogrel) ADP-induced platelet aggregation, we hypothesized that on-treatment platelet reactivity may be a better predictor of post-stenting ischemic events than responsiveness to clopidogrel (8). Since 2005 numerous investigations have reported a relationship between high on-treatment platelet reactivity to ADP and in-hospital, 6-month, 1-year, and 2-year post-stenting ischemic risk including stent thrombosis (6,9-14). In this issue of the Journal, Sibbing et al. ( 15) report the results of a large 2-center prospective study designed to investigate the relationship between platelet reactivity to ADP and the 30-day cumulative incidence of definite stent thrombosis as defined by the Academic Research Consortium. The authors measured platelet reactivity with a new impedance aggregometer also known as the Multiplate analyzer (Dynabyte, Munich, Germany). This device measures aggregation in whole blood, thus enhancing the ease of measurement by obviating centrifugation as required by LTA. The same authors have previously reported that Multiplate measurements correlate with LTA, the most widely utilized technique in translational research studies that have associated platelet reactivity with post-stenting ischemic risk ( 16). The highest quintile was used as the pre-specified cut point for high platelet reactivity, termed clopidogrel low responders by the authors and used to size the study. However, the latter term is somewhat misleading because assessment of clopidogrel responsiveness requires a pre-treatment measurement of platelet function, a measurement that was absent in the current study. Platelet function was determined only once in the catheterization laboratory and associated with the occurrence of 30-day stent thrombosis. There were 7 definite stent thromboses in the clopidogrel low responders and 3 in the clopidogrel responders. The association of a single measurement with the occurrence of a post-stent thrombotic event is the most commonly reported link in the literature. Currently, there is an enormous void in our knowledge regarding the stability of the high platelet reactivity phenotype. Serial measurements of platelet function are lacking in the literature and in the current article. In a similar fashion to other studies (6,10), Sibbing et al. (15) performed a receiver-operator characteristic (ROC) curve analysis to determine the optimal platelet function cut point associated with stent thrombosis. They identified a cut point of 468 AU as the best discriminatory threshold, yielding an area under the curve of 0.78 for the prediction of stent thrombosis. The aforementioned finding was similar to a recent study using LTA, in which an ROC analysis yielded an area under the curve of 0.78 for 2-year post-stent ischemic events (10). It should be noted that the Sibbing et al. (15) study involved a very heterogeneous group of patients who received various parenteral antithrombotic regimens for different clinical presentations. Although clinical presentation of coronary artery disease was evaluated as a potential confounder in the Cox regression model, parenteral antiplatelet therapy was not, and therefore a potential independent predictive value of the latter is unknown. Moreover, patients were loaded with clopidogrel irrespective of maintenance therapy. The timing of platelet function measurements was also similarly highly variable, but was performed at least 2 h after clopidogrel loading. Prior investigations have clearly shown that an assessment of clopidogrel response is dependent on dose and the time at which platelet function is measured after treatment. It is therefore not surprising that clopidogrel low-responsive patients had a shorter interval of time between loading and platelet function analyses. Determining whether patients treated with clopidogrel for sufficient time to allow a pharmacodynamic effect and who have high platelet reactivity measured by a point-of-care device are truly at risk for a thrombotic event is of major importance in this field of investigation. It is curious that despite not allowing maximum platelet inhibition by clopidogrel to occur in all patients before platelet function analyses, the investigators still found a relationship between their measurement and the primary end point. It is unknown whether the relationship would remain the same if platelet function measurements were conducted at a uniform pre-specified time allowing the full antiplatelet effect of clopidogrel. Have the investigators successfully answered the two burning questions with their investigation? They must be congratulated for showing an association between a cutoff value of high platelet reactivity measured by a point-of-care device and the occurrence of stent thrombosis in a large study. Their study further strengthens the hypothesis that ischemic events largely occur above a threshold of platelet reactivity to ADP as measured by an ex vivo method. However, given the above limitations, whether ischemic event occurrence is primarily explained by high on-treatment platelet reactivity to ADP remains incompletely answered. We believe that caution is warranted in extrapolating the results of this study to different patient populations and in guiding individualized antiplatelet therapy. Furthermore, this study lacks adequate power to assess the association between platelet reactivity and bleeding. Thus, the second question of whether bleeding is primarily explained by low platelet reactivity remains unanswered. The work of Sibbing et al. (15) is definitely a major step forward to unraveling the mystery of why selected post-stent patients bleed whereas others suffer the dreaded coronary artery thrombotic event. Continued translational research holds the promise of marked improvements in clinical outcomes guided by objective measurements of platelet physiology in the individual patient. The ultimate goal would be the potential identification of a therapeutic window for P2Y12 receptor blockade as shown in Figure. The current available data suggest that post-stenting ischemic events are associated with a P2Y12 reactivity cut point. However, there is a very large gap in our understanding of the relationship of P2Y12 reactivity to bleeding.
References
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||