| Text |
Comprehensive
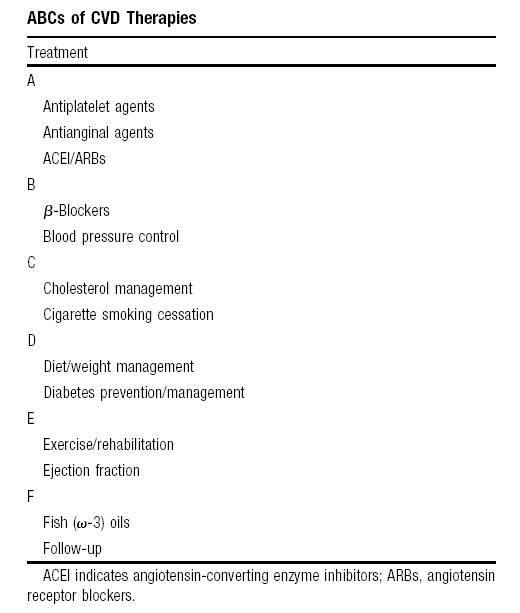
risk-factor management is the cornerstone of therapy in women
and men with known cardiovascular disease (CVD). Therapeutic interventions
can be summarized in an "ABC" format (Table).13 CVD death
rates have declined in men and older women during the past
decade.4 By contrast, there has been a significant rise
in CVD deaths among younger women.5 Evidence-based therapies,
including aspirin use, have been believed to account for half
of the decline in CVD death rates, whereas improvement in risk
factors, including lower cholesterol and blood pressure, accounts
for the other half.6
The
use of aspirin in medicine dates at least as far back as Hippocrates,
who found analgesic effects for the extract (salicin) of white
willow bark.7 Aspirin irreversibly inactivates platelet
cyclooxygenase, preventing platelets from synthesizing thromboxane
A2, a potent vasoconstrictor and promoter of platelet
aggregation. Aspirin also has anti-inflammatory and vasodilatory
effects that may be important.
Over
the past 3 decades, aspirin has been shown to decrease the
risk of CVD events and mortality in clinical trials of men and
women with CVD.8 The latest meta-analysis by the Antiplatelet
Trialists collaboration in 2002 analyzed 135 000 patients
with CVD. Compared with placebo, antiplatelet therapy (mostly
aspirin) resulted in a relative risk reduction of about one
quarter for CVD events, one third for nonfatal myocardial infarction,
one quarter for stroke, and 15% for CVD mortality.9 Antiplatelet
therapy reduced the relative risk of ischemic stroke by 30%
but increased the relative risk of hemorrhagic stroke by 22%.9
Because ischemic stroke was more common than hemorrhagic stroke,
the absolute benefit was greater than the absolute risk of antiplatelet
therapy, with a net relative risk reduction of total stroke
by 22%. In 3 trials (N=3570) that directly compared a dose 75
mg daily versus <75 mg, there was no statistically significant
difference between the doses. Aspirin doses of 75 to 150 mg
had as much benefit as higher doses (160 to 1500 mg). Insufficient
data were available on those treated with <75 mg to provide
definitive recommendations on the use of <75 mg daily.9
One
limitation of the 2002 meta-analysis is the lack of sex-specific
or age-specific subgroup data. In the previous 1994 meta-analysis
by the Antiplatelet Trialists, sex-specific data were analyzed
from 29 trials with 40 000 men and 10 000 women with known CVD.8
Women derived as much benefit as did men from aspirin.8
In
patients without known CVD, the picture is less clear. In the
primary prevention setting, aspirin reduces the risk of myocardial
infarction but not stroke in men, and reduces the risk of stroke
but not myocardial infarction in women.10,11 There has been
little or no benefit for aspirin in reducing death (CVD or
all cause) in men or women without known CVD. Aspirin did not
prevent CVD in asymptomatic Japanese patients with diabetes
in the primary prevention setting unless they were age 65 or
older.12 Guidelines recommend using aspirin for primary
prevention in higher risk men and women who have increased event
rates and a greater benefit-to-risk ratio.13
In
this issue of Circulation: Cardiovascular Quality and Outcomes,
Berger et al14 examined aspirin use and dose in relation
to clinical outcomes in 8928 postmenopausal women with known
CVD followed up for 6.5 years in the Womens Health Initiative
(WHI) Observational Study. After controlling for potential confounders,
women who reported taking aspirin at least 3 times a week had
significant risk reductions in all-cause death (14%) and CVD
death (25%) compared with nonusers. There was also a 10% risk
reduction in composite CVD events (including nonfatal myocardial
infarction) that did not reach statistical significance. An
aspirin dose of 81 mg was comparable with 325 mg for preventing
clinical events in 2072 women who were matched on risk factors
and other potential confounders.
Although
the present WHI study is an observational study, it adds to
previous findings from randomized clinical trials. The use
of propensity scores to control for confounding may not completely
balance unmeasured confounders as would randomization in a
clinical trial, but it may reduce confounding when determinants of
drug use are multifactorial, as in the case of aspirin.15 The
magnitude of the benefit associated with aspirin use was similar
to the estimates obtained from meta-analyses of clinical trials,
as was the consistency of benefit with lower versus higher
doses of aspirin for preventing clinical outcomes.8,9
Finally,
the most striking finding of this WHI study is the low use
of aspirin and other proven therapies in community women with
known CVD (19941998). Less than 1 in 2 women in the study
were taking aspirin, and rates were lower in black women and
those with Medicaid insurance. Statin and β-blocker use
in the study was even lower than aspirin, with <1 in 4 women
taking statins or β-blockers, a rate similar to their
use of nonsteroidal anti-inflammatory drugs.
We
learned from the WHI and Heart and Estrogen/Progestin Replacement
Study randomized clinical trials that estrogen and progesterone
therapy did not confer cardiovascular protection and may increase
CVD risk in postmenopausal women.16,17 An important lesson
from this WHI observational study is that lifesaving therapies,
including aspirin, β-blockers, and statins, continue to
be substantially underused in postmenopausal women with known
CVD. Our greatest challenge remains the wider implementation
of the ABCs of CVD treatment and prevention in both men and
women.
Sources
of Funding
Dr
Mora has received research grant support from the American Heart
Association (0670007N), the National Heart, Lung, and Blood
Institute (K08 HL094375), the Sandra A. Daugherty Foundation, a
Lerner Research Young Investigator Award, Merck, and AstraZeneca
and speaking honorarium from Pfizer for an educational (nonpromotional)
activity.
References
1. Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas
JS, Ferguson TB Jr, Fihn SD, Fraker TD Jr, Gardin JM, O'Rourke RA, Pasternak
RC, Williams SV, Alpert JS, Antman EM, Hiratzka LF, Fuster V, Faxon DP,
Gregoratos G, Jacobs AK, Smith SC Jr. ACC/AHA 2002 guideline update for
the management of patients with chronic stable angina: summary article:
a report of the American College of Cardiology/American Heart Association
Task Force on Practice Guidelines (Committee on the Management of Patients
With Chronic Stable Angina). Circulation. 2003; 107: 149158.
2.
Fraker TD Jr, Fihn SD, Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania
PC, Douglas JS, Ferguson TB Jr, Gardin JM, O'Rourke RA, Williams SV, Smith
SC Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger
SM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura
R, Page RL, Riegel B, Tarkington LG, Yancy CW. 2007 chronic angina focused
update of the ACC/AHA 2002 Guidelines for the management of patients with
chronic stable angina: a report of the American College of Cardiology/American
Heart Association Task Force on Practice Guidelines Writing Group to develop
the focused update of the 2002 guidelines for the management of patients
with chronic stable angina. Circulation. 2007; 116: 27622772.
3.
Gluckman TJ, Baranowski B, Ashen MD, Henrikson CA, McAllister M, Braunstein
JB, Blumenthal RS. A practical and evidence-based approach to cardiovascular
disease risk reduction. Arch Intern Med. 2004; 164: 14901500.
4.
Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal
K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard
V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott
M, Meigs J, Mozaffarian D, Nichol G, O'Donnell C, Roger V, Rosamond W,
Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller
S, Wong N, Wylie-Rosett J, Hong Y. Heart disease and stroke statistics2009
update: a report from the American Heart Association Statistics Committee
and Stroke Statistics Subcommittee. Circulation. 2009; 119: 480486.
5.
Ford ES, Capewell S. Coronary heart disease mortality among young adults
in the U.S. from 1980 through 2002: concealed leveling of mortality rates.
J Am Coll Cardiol. 2007; 50: 21282132.
6.
Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles
WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease,
19802000. N Engl J Med. 2007; 356: 23882398.
7.
Kurth T, Buring JE, Ridker PM, Gaziano JM. Aspirin, other antiplatelet
agents, and anticoagulants. In: Manson JE, Buring J, Ridker P, Gaziano
M, eds. Clinical Trials in Cardiovascular Disease: A Companion to Braunwalds
Heart Disease. 2nd ed. Philadelphia, Pa: WB Saunders; 2004: 333348.
8.
Collaborative overview of randomised trials of antiplatelet therapy. I.
Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet
therapy in various categories of patients. Antiplatelet Trialists Collaboration.
BMJ. 1994; 308: 81106.
9.
Collaborative meta-analysis of randomised trials of antiplatelet therapy
for prevention of death, myocardial infarction, and stroke in high risk
patients. BMJ. 2002; 324: 7186.
10.
Ridker PM, Cook NR, Lee IM, Gordon D, Gaziano JM, Manson JE, Hennekens
CH, Buring JE. A randomized trial of low-dose aspirin in the primary prevention
of cardiovascular disease in women. N Engl J Med. 2005; 352: 12931304.
11.
Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL.
Aspirin for the primary prevention of cardiovascular events in women and
men: a sex-specific meta-analysis of randomized controlled trials. JAMA.
2006; 295: 306313.
12.
Ogawa H, Nakayama M, Morimoto T, Uemura S, Kanauchi M, Doi N, Jinnouchi
H, Sugiyama S, Saito Y; for the Japanese Primary Prevention of Atherosclerosis
With Aspirin for Diabetes (JPAD) Trial Investigators. Low-dose aspirin
for primary prevention of atherosclerotic events in patients with type
2 diabetes: a randomized controlled trial. JAMA. 2008; 300: 21342141.
13.
Mosca L, Banka CL, Benjamin EJ, Berra K, Bushnell C, Dolor RJ, Ganiats
TG, Gomes AS, Gornik HL, Gracia C, Gulati M, Haan CK, Judelson DR, Keenan
N, Kelepouris E, Michos ED, Newby LK, Oparil S, Ouyang P, Oz MC, Petitti
D, Pinn VW, Redberg RF, Scott R, Sherif K, Smith SC Jr, Sopko G, Steinhorn
RH, Stone NJ, Taubert KA, Todd BA, Urbina E, Wenger NK. Evidence-based
guidelines for cardiovascular disease prevention in women: 2007 update.
Circulation. 2007; 115: 14811501.
14.
Berger JS, Brown DL, Burke GL, Oberman A, Kostis JB, Langer RD, Wong ND,
Wassertheil-Smoller S. Aspirin use, dose, and clinical outcomes in postmenopausal
women with stable cardiovascular disease: the Womens Health Initiative
Observational Study. Circ Cardiovasc Qual Outcomes. 2009; 2: 7887.
15.
Glynn RJ, Schneeweiss S, Sturmer T. Indications for propensity scores
and review of their use in pharmacoepidemiology. Basic Clin Pharmacol
Toxicol. 2006; 98: 253259.
16.
Hulley S, Grady D, Bush T, Furberg C, Herrington D, Riggs B, Vittinghoff
E. Randomized trial of estrogen plus progestin for secondary prevention
of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin
Replacement Study (HERS) Research Group. JAMA. 1998; 280: 605613.
17.
Manson JE, Hsia J, Johnson KC, Rossouw JE, Assaf AR, Lasser NL, Trevisan
M, Black HR, Heckbert SR, Detrano R, Strickland OL, Wong ND, Crouse JR,
Stein E, Cushman M. Estrogen plus progestin and the risk of coronary heart
disease. N Engl J Med. 2003; 349: 523534.
|
