| Text |
In
The Lancet today, the Antithrombotic Trialists' (ATT) Collaboration reports
on an individual participant data meta-analysis of primary prevention
with aspirin.1 The ATT investigators should be commended for this labour-intensive
work on more than 95 000 individuals from six randomised clinical trials.
The main added value of the present report compared with an earlier aggregate
data meta-analysis on the same six trials is that it had access to individual
participant data,2 which allowed the ATT investigators to estimate the
magnitude of several risk factors for selected outcomes. Factors such
as age, male sex, diabetes mellitus, and high blood pressure were not
only associated with ischaemic complications, but also with bleeding,
although somewhat less strongly. The ATT investigators reported that the
risk of serious vascular events dropped from 0·57% to 0·51%
per year by the use of aspirin, but that it increased the risk of major
bleeds from 0·07% to 0·10% per year. They therefore concluded
that aspirin is of uncertain value for primary prevention.
A major difference in reporting between the two studies is that the investigators
of the aggregate data meta-analysis primarily reported effectiveness data
for women and men separately, whereas the present report does not. The
ATT investigators do provide these data, but reasoned that the proportional
reduction in specific vascular outcomes did not differ significantly between
men and women when adjustment for multiple comparisons was made. Hence,
they do not differentiate between women and men in their recommendations.
Is this the optimum approach? First, at the level of single comparisons
there were several tests for the different effects of aspirin in women
and men that were significant. For major coronary events, the p value
for heterogeneous effectiveness between the sexes was 0·03, that
for first stroke (any type) was 0·004, and that for probable ischaemic
stroke was 0·005. The latter two remained significant when the
ATT global test for heterogeneity was used. The ATT investigators, however,
dismissed these differences with the use of a strict multiple comparisons
criterion, whereas published work for multiple comparisons is at least
as heterogeneous itself.3—5 Second, the ATT investigators obtained
information from secondary prevention trials in which different effects
of aspirin between the sexes were virtually absent. We think that one
should be very cautious with borrowing of data from patients with clinically
manifest disease. We are therefore not willing to give the secondary prevention
data as much weight in the assessment of the primary prevention data as
the ATT investigators do. Third, incidence rates of myocardial infarction,
ischaemic stroke, intracranial haemorrhage, and gastrointestinal bleeding
differ between the sexes, which affects the balance between benefits and
risks.
How can we use today's study in daily practice? For example, should the
first author of this Comment (55-year-old man, slightly elevated cholesterol,
no other vascular risk factors) take an aspirin a day to keep the doctor
away? The ATT investigators try to balance benefits (less serious vascular
events) and risks (more haemorrhages), but without taking into account
the consequences of both harms and benefits on quality of life.
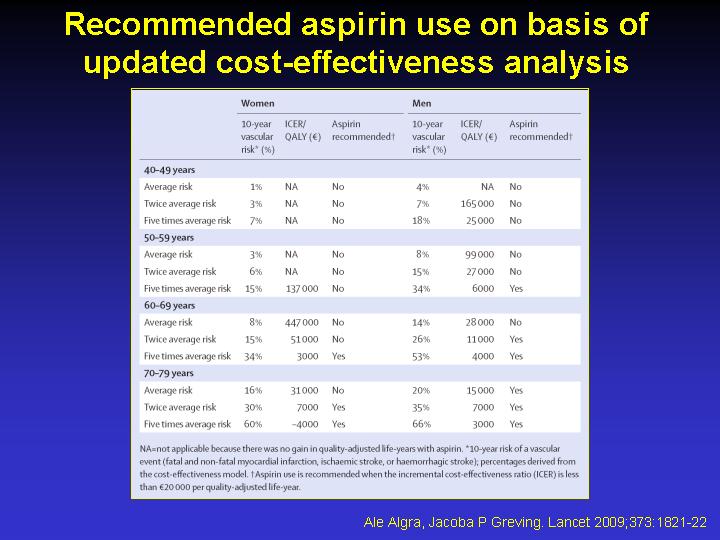
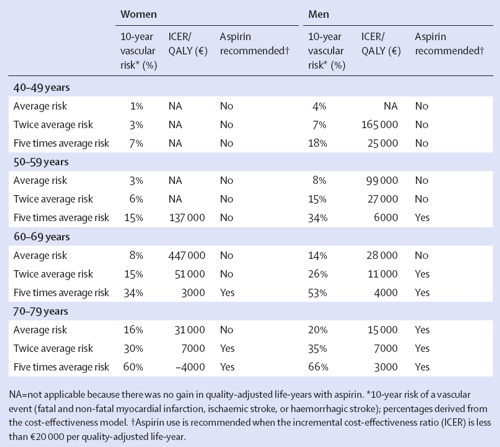
We thus decided to update our previous cost-effectiveness analysis6 with
the new data provided by the ATT investigators. We have used the slightly
different risk ratios for cardiac events and ischaemic stroke for women
and men separately. Moreover, in individuals for whom we used an increased
risk of cardiovascular disease we let the risk of haemorrhage increase
proportionally on the basis of the new ATT observations. The table summarises
for which individuals an incremental cost-effectiveness ratio of €20
000 or less would be obtained; these individuals are probably the best
candidates for prevention with aspirin. These ratios are the most reliable
estimates since all data have been incorporated in the cost-effectiveness
analysis, but these ratios come with their own uncertainty (see the sensitivity
analysis in table 5 of our previous report).6 The new estimates from the
cost-effectiveness analysis imply that the first author does not need
to take an aspirin a day. It should be emphasised that our model also
took the (dis)utility of taking aspirin into account and our sensitivity
analyses indicated that the results of our analyses were sensitive to
it. Patients might not wish to be medicalised7—such considerations
are important in the decision to take aspirin or not. Whether statins
should be preferred above aspirin is a different and difficult question
that needs careful consideration too. Apart from drug treatment, one must
not forget the importance of lifestyle changes, such as cessation of smoking,
healthy diet, and regular exercise.
Recommended
aspirin use on basis of updated cost-effectiveness analysis6
References
1 Antithrombotic Trialists' (ATT) Collaboration. Aspirin in the primary
and secondary prevention of vascular disease: collaborative meta-analysis
of individual participant data from randomised trials. Lancet 2009; 373:
1849-1860.
2 Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown
DL. Aspirin for the primary prevention of cardiovascular events in women
and men: a sex-specific meta-analysis of randomized controlled trials.
JAMA 2006; 295: 306-313.
3 Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology
1990; 1: 43-46.
4 Bland JM, Altman DG. Multiple significance tests: the Bonferroni method.
BMJ 1995; 310: 170.
5 Perneger TV. What's wrong with Bonferroni adjustments. BMJ 1998; 316:
1236-1238.
6 Greving JP, Buskens E, Koffijberg H, Algra A. Cost-effectiveness of
aspirin treatment in the primary prevention of cardiovascular disease
events in subgroups based on age, gender and varying cardiovascular risk.
Circulation 2008; 117: 2875-2883.
7 Christie B. Guidelines on treating risk factors turn healthy people
into patients, doctors say. BMJ 2006; 333: 988.
E' disponibile un set di diapositive tratte dall'articolo:
alert-08-Lancet_2009_373_1821.ppt
(222 KB)

|