ascot.zip (241Kb)
![]()

ASCOT lipid arm shows 36% reduction in primary end point
Chicago, IL - Lipid lowering with atorvastatin significantly
reduced the risk of major cardiovascular events in hypertensive patients
with normal cholesterol levels in the Anglo-Scandinavian Cardiac
Outcomes Trial (ASCOT).
The trial was presented at the American
College of Cardiology 2003 Scientific Sessions on Wednesday April
2 by study cochairs Drs Peter Sever (Imperial College,
London) and Bjorn Dahlöf (Sahlgrenska University Hospital,
Gothenburg, Sweden) and simultaneously published online in the Lancet.[1]
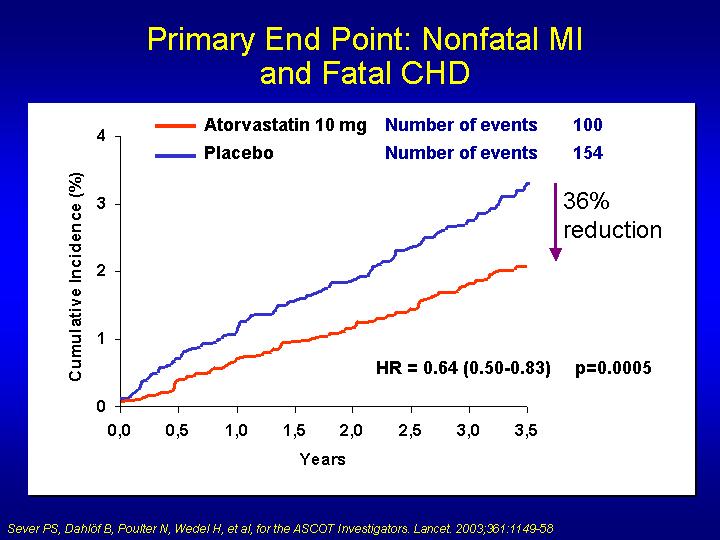
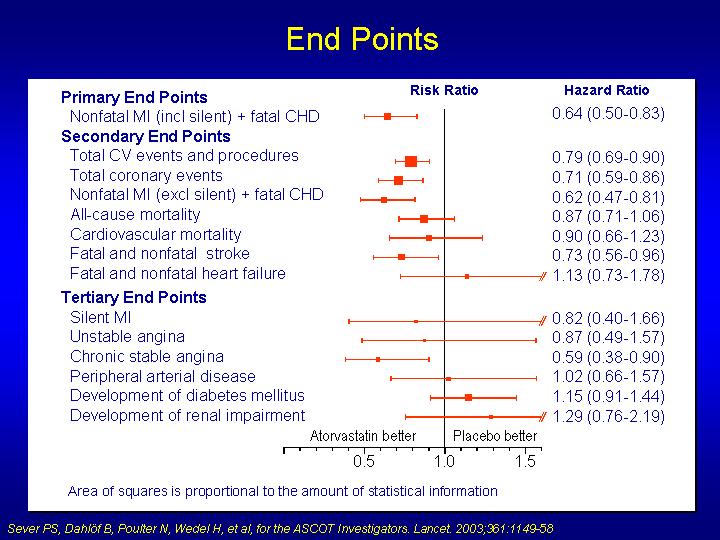
Results showed a significant 36% reduction in
the primary end point of fatal CHD/nonfatal MI in the atorvastatin group
after a median follow-up of 3.3 years. Dahlöf concluded that: "The
reduction in events is large, given the relatively short-term follow-up
and occurred earlier than in other statin trials. These results should
therefore have implications for future guidelines."
"A very important study"
Chair of the ACC hotline session Dr Bertram
Pitt (University of Michigan, Ann Arbor) said: "This is
obviously a very important study and should have a marked influence on
clinical practice." But, he added: "Since we do such a poor
job with blood pressure in hypertensive patients, how can we expect these
results to be implemented?"
Outlining the background and rationale of the
study, Sever explained that although lowering cholesterol in individuals
at high risk of cardiovascular disease is well known to improve outcome,
cholesterol lowering in the primary prevention of coronary heart disease
in hypertensive patients with normal cholesterol levels has not been assessed.
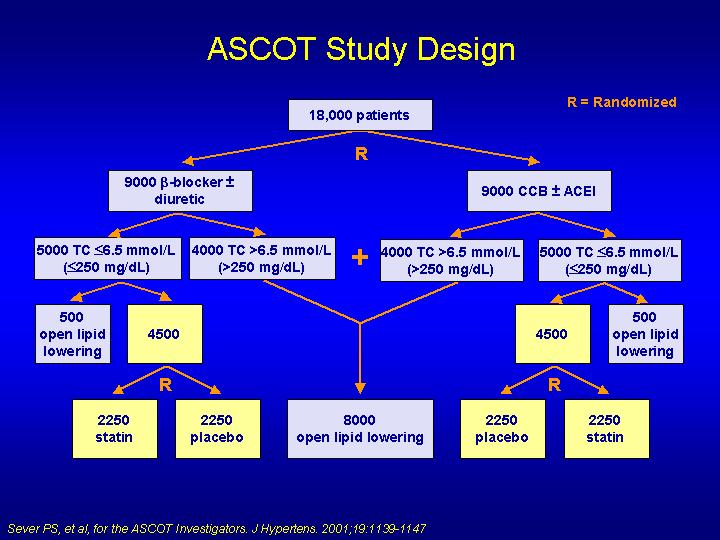
The ASCOT trial is made up of two studies in hypertensive
patients a comparison of two different antihypertensive
regimens (which is still ongoing), and a lipid-lowering study.
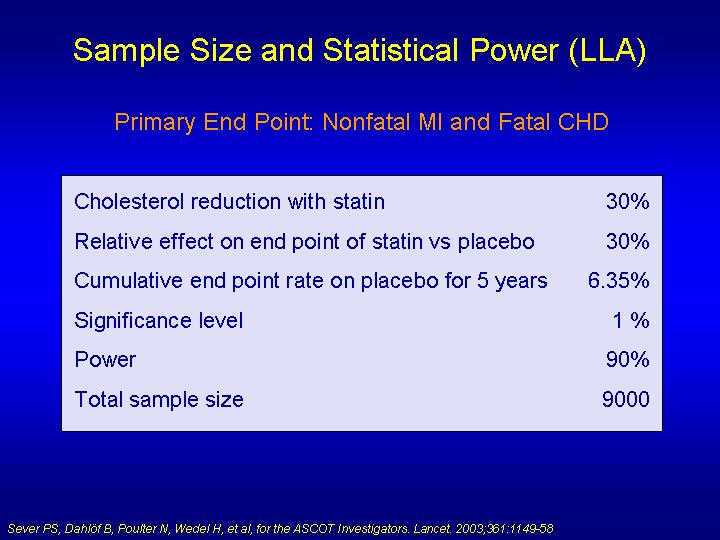
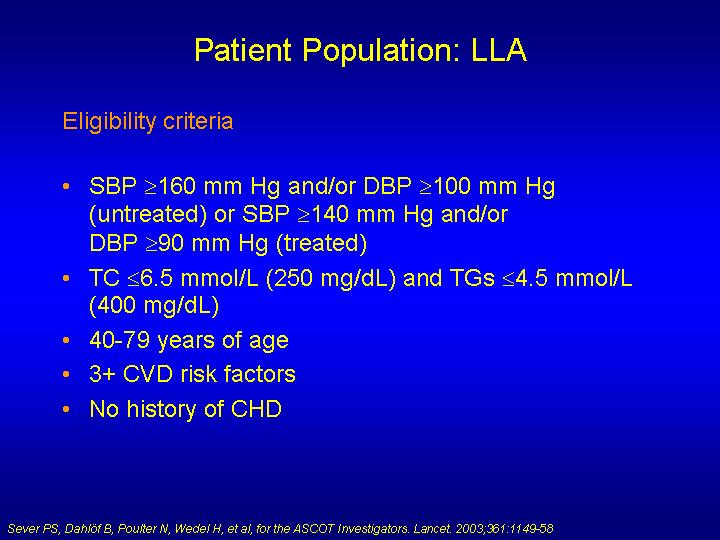
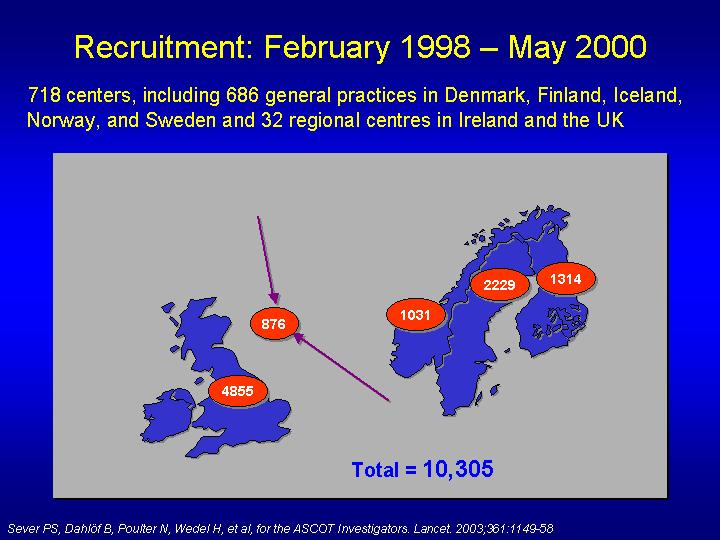
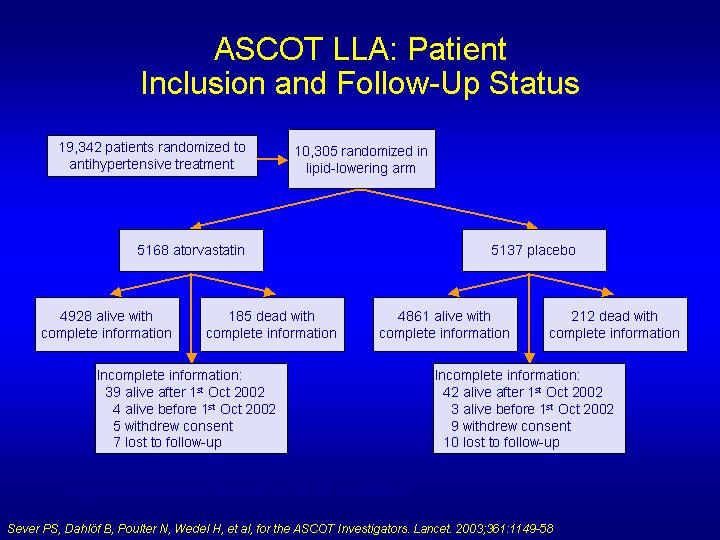
The lipid part of the ASCOT trial involved 10 305
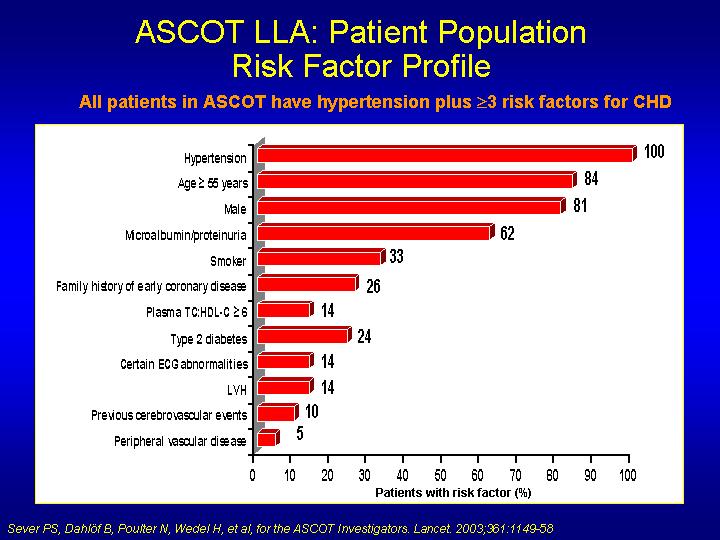
hypertensive patients aged 40 to 79 years with at least three other cardiovascular
risk factors and with total cholesterol below 6.5 mmol/L (250 mg/dL).
They were randomized to 10-mg atorvastatin or placebo. Follow-up was planned
for 5 years, but treatment was stopped after 3.3 years because of significant
benefits in the atorvastatin group.
This benefit emerged in the first year of follow-up.
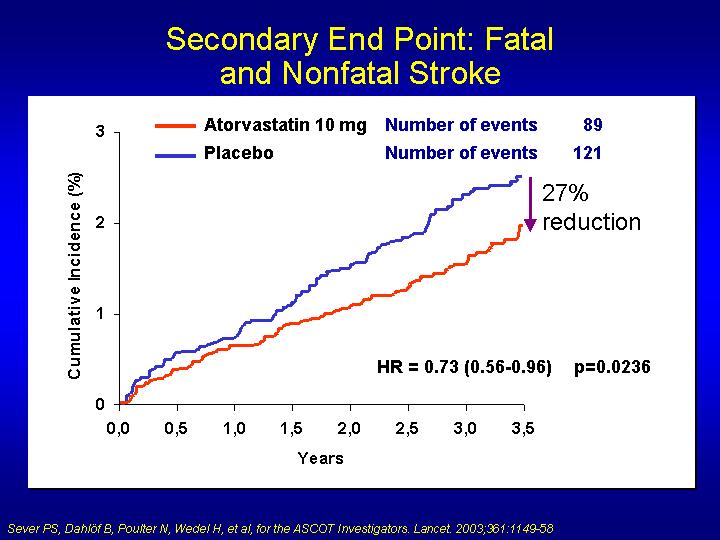
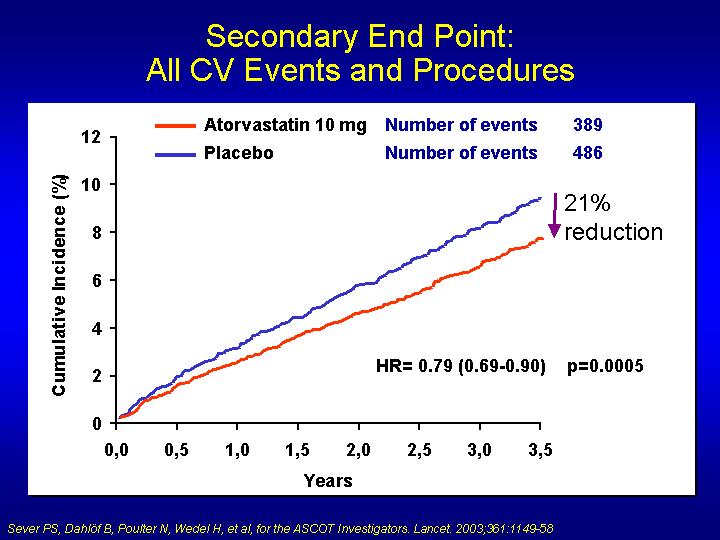
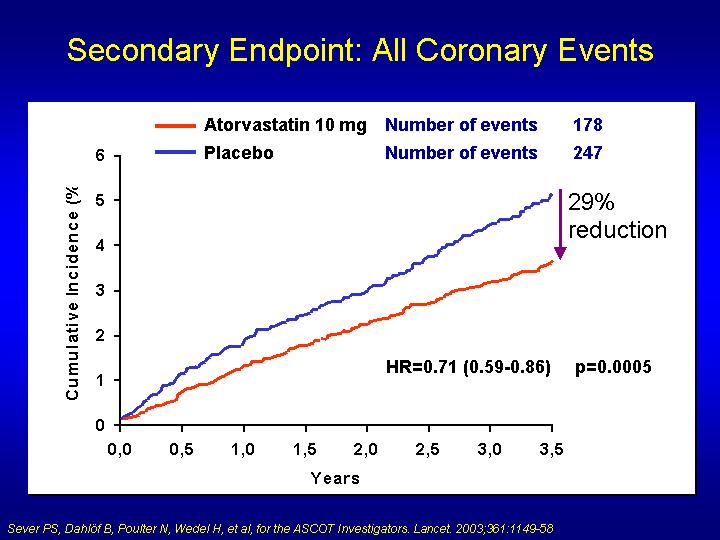
As well as a reduction in the primary end point, fatal and nonfatal stroke,
total cardiovascular events, and total coronary events were also significantly
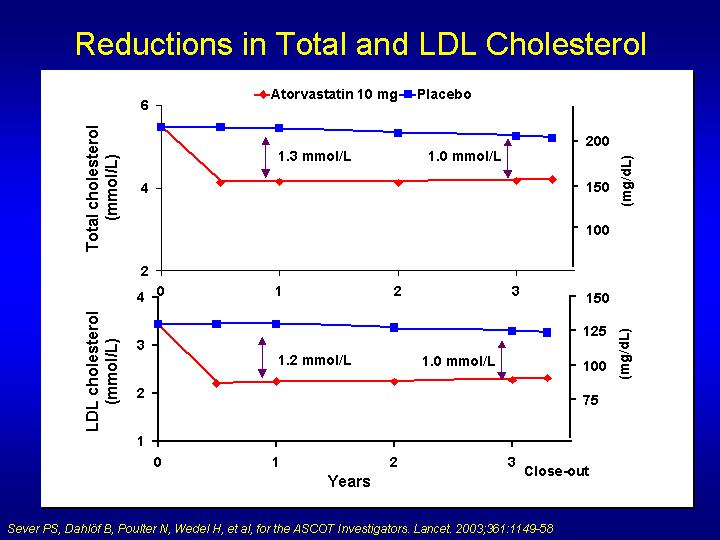
lowered. Atorvastatin lowered total serum cholesterol by about 1.3 mmol/L
compared with placebo at 12 months and by 1.1 mmol/L after three years
of follow-up.
ASCOT primary end point
|
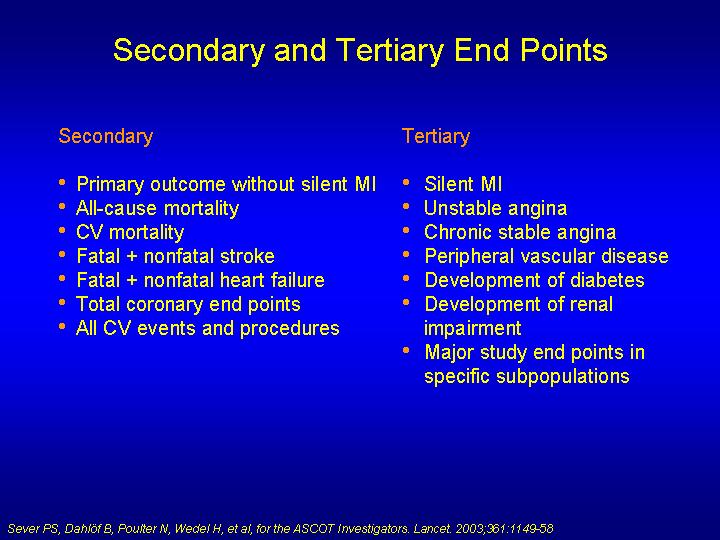
ASCOT secondary end points
|
ASCOT tertiary end points
|
Benefits would have been larger with longer follow-up
In the discussion section of the Lancet
paper, the authors note that after one year of follow-up in ASCOT, total
cholesterol and LDL cholesterol among patients taking atorvastatin were
24% and 35% lower, respectively, than among those taking placebo. They
point out that the dose of atorvastatin was not titrated up in ASCOT,
although higher doses would have resulted in greater reductions in total
cholesterol and LDL-cholesterol concentrations and would probably have
produced even larger reductions in cardiovascular events. "Had the
study continued for an average follow-up of five years, as originally
planned, the reduction in fatal and nonfatal CHD events may have approached
50%," they add.
The researchers say that the small increases in
life-threatening arrhythmias, heart failure, renal impairment, and new-onset
diabetes seen in the atorvastatin group were based on small numbers of
events and are probably the result of chance variation.
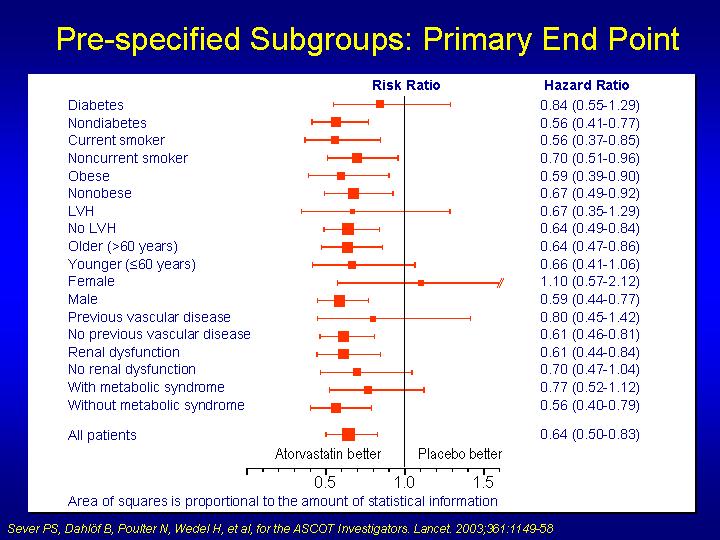
Noting that the relative reduction in the primary
end point was less in patients with diabetes than those without might
be thought of as "surprising," they point out that as there
were only 84 events in patients with diabetes, this finding may well reflect
inadequate power. The higher use of statins among patients with diabetes
assigned placebo (14%) compared with nondiabetics (8%) may have also been
a factor, they add.
There was also an apparent lack of significant
benefit of atorvastatin on the primary end point among women. The ASCOT
investigators again attribute this to the small number of events (36)
in this group, adding that this highlights a potential shortcoming of
the trial, which included mainly white male participants.
Comparison with ALLHAT
ASCOT is similar to the recently reported US ALLHAT
trial, which also looked at both antihypertensive and lipid-lowering treatment
in hypertensive patients. In the lipid arm of ALLHAT, 10 355 hypertensive
patients were randomized to 40-mg pravastatin or usual care. The ASCOT
investigators point out that the baseline demographics of patients included
in the lipid-lowering arm of ALLHAT differ substantially from those in
ASCOT ALLHAT included a slightly older cohort,
of whom about 14% had a history of CHD, and a notably greater proportion
of women and nonwhite people.
No significant benefits in terms of all-cause
mortality or coronary and stroke events were apparent with statin use
in ALLHAT. This has been explained by substantial use of statins in the
usual-care group, leading to differences in total cholesterol and LDL
cholesterol of only 9% and 17%, respectively, between the two groups.
In contrast, in ASCOT only 9% of patients in the placebo group were using
statins by three years of follow-up, which the authors say correlates
with the fact that lipid concentrations and risk profiles of patients
were lower than those at which statin therapy is currently recommended.
In addition, only 13% of patients assigned to atorvastatin dropped out
of this treatment group at three years, thus maintaining the integrity
and power of the original study design.
Benefits additional to blood pressure reductions
The reduction in all-cause mortality in ASCOT
(13%) was very similar to that seen in the blood-pressure-lowering trials
(12%), but the authors note that the benefits of statin treatment are
additional to those of good blood-pressure control. "Consequently,
more serious consideration now needs to be given to the most resource-effective
way of providing both of these risk-factor intervention strategies to
hypertensive patients to prevent fatal and nonfatal cardiovascular events."
"Our findings add further support to the
concept that treatment strategies to reduce cardiovascular disease should
depend on global assessment of risk rather than on numerical values of
individual risk factors and that benefits of lipid lowering are apparent
across the whole range of serum cholesterol concentrations," they
add.
Absolute benefit limited?
In an accompanying Lancet commentary, Drs
Lars Lindholm (Umeå University, Sweden) and Ola Samuelsson
(Göteborg University, Sweden) note that while the ASCOT trial showed fairly
large relative reductions in cardiovascular events associated with active
lipid-lowering therapy, the absolute benefits are not so impressive.[2]
"In absolute terms the difference between
active treatment and placebo in the incidence of cardiovascular disease
was only 3.4 per 1000 patient-years for the primary event and 2.0 per
1000 patient-years for stroke. Hence, active lipid-lowering treatment
can be estimated to result in only a small increase in the probability
of remaining free from a myocardial infarction over five years, from 95%
to 97%, in patients with good control of blood pressure," they write.
"The ASCOT investigators hope that their
data will have implications for future lipid-lowering guidelines. However,
any guideline changes should be left to the guidelines committees to decide,
when they balance the limited absolute benefits against the treatment
cost of lipid lowering," Drs Lindholm and Samuelsson conclude.
|
Sources |
|
|
|
|
|
|
|
|
Fonte: Sue Hughes,
theheart.org