| Authors |
The DREAM Trial Investigators |
|
| Title |
Effect of Ramipril on the Incidence of Diabetes |
|
| Full source | N Engl J Med. 2006 Sep 15; [Epub ahead of print] | |
|
|
Per scorrere le diapositive |
|
|
||
| Abstract |
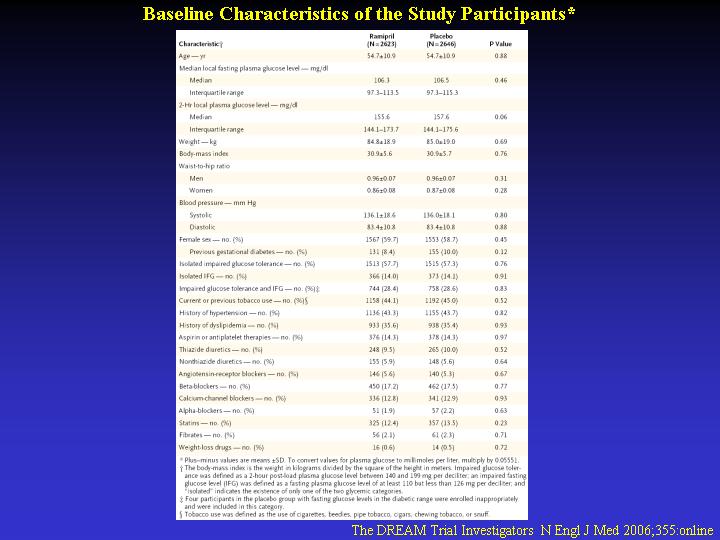
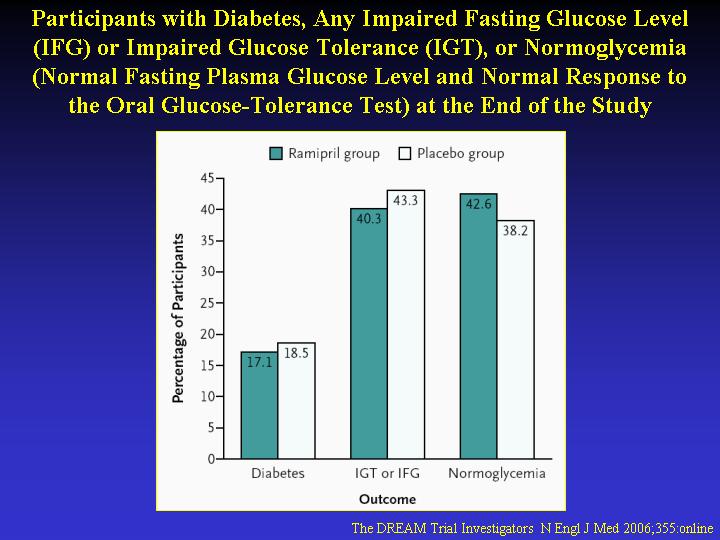
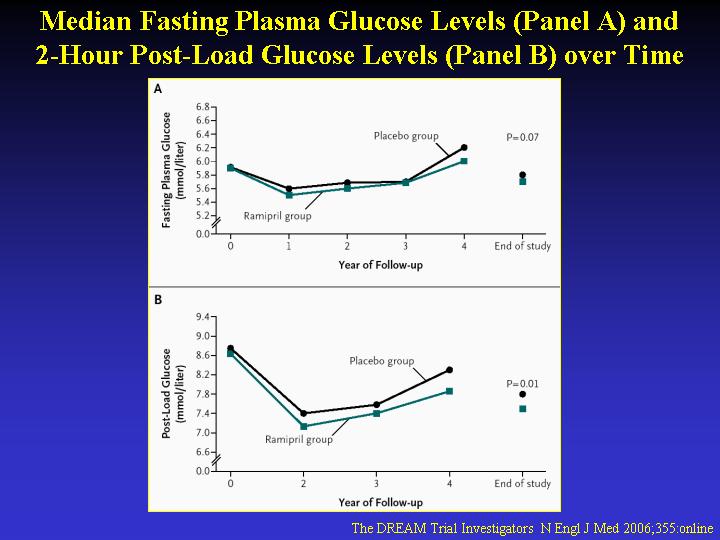
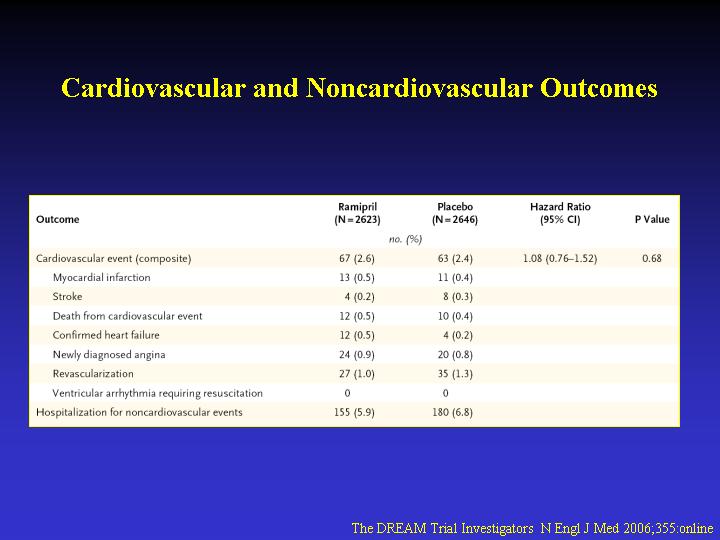
Background Previous studies have suggested that blockade of the renin-angiotensin system may prevent diabetes in people with cardiovascular disease or hypertension. Methods In a double-blind, randomized clinical trial with a 2-by-2 factorial design, we randomly assigned 5269 participants without cardiovascular disease but with impaired fasting glucose levels (after an 8-hour fast) or impaired glucose tolerance to receive ramipril (up to 15 mg per day) or placebo (and rosiglitazone or placebo) and followed them for a median of 3 years. We studied the effects of ramipril on the development of diabetes or death, whichever came first (the primary outcome), and on secondary outcomes, including regression to normoglycemia. Results The incidence of the primary outcome did not differ significantly between the ramipril group (18.1%) and the placebo group (19.5%; hazard ratio for the ramipril group, 0.91; 95% confidence interval [CI], 0.81 to 1.03; P=0.15). Participants receiving ramipril were more likely to have regression to normoglycemia than those receiving placebo (hazard ratio, 1.16; 95% CI, 1.07 to 1.27; P=0.001). At the end of the study, the median fasting plasma glucose level was not significantly lower in the ramipril group (102.7 mg per deciliter [5.70 mmol per liter]) than in the placebo group (103.4 mg per deciliter [5.74 mmol per liter], P=0.07), though plasma glucose levels 2 hours after an oral glucose load were significantly lower in the ramipril group (135.1 mg per deciliter [7.50 mmol per liter] vs. 140.5 mg per deciliter [7.80 mmol per liter], P=0.01). Conclusions Among persons with impaired fasting glucose levels or impaired glucose tolerance, the use of ramipril for 3 years does not significantly reduce the incidence of diabetes or death but does significantly increase regression to normoglycemia. (ClinicalTrials.gov number, NCT00095654.) Notice: To coincide with an author presentation at the European Association for the Study of Diabetes meeting, this article was published at www.nejm.org on September 15, 2006. It will appear in the October issue of the Journal.
|
|