| Authors |
Bibbins-Domingo K, Gupta R, Na B, Wu AH, Schiller NB, Whooley MA. |
|
| Title |
N-terminal fragment of the prohormone brain-type natriuretic peptide (NT-proBNP), cardiovascular events, and mortality in patients with stable coronary heart disease |
|
| Full source | JAMA 2007;297:169-76 | |
|
|
Per scorrere le diapositive |
|
|
||
| Abstract |
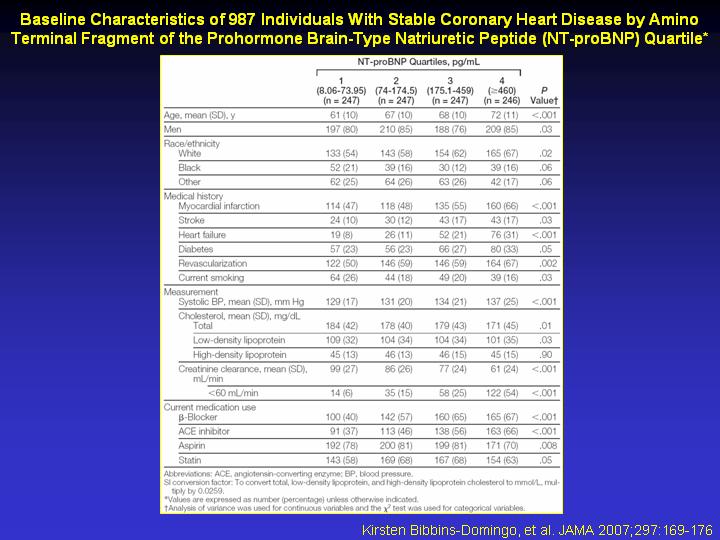
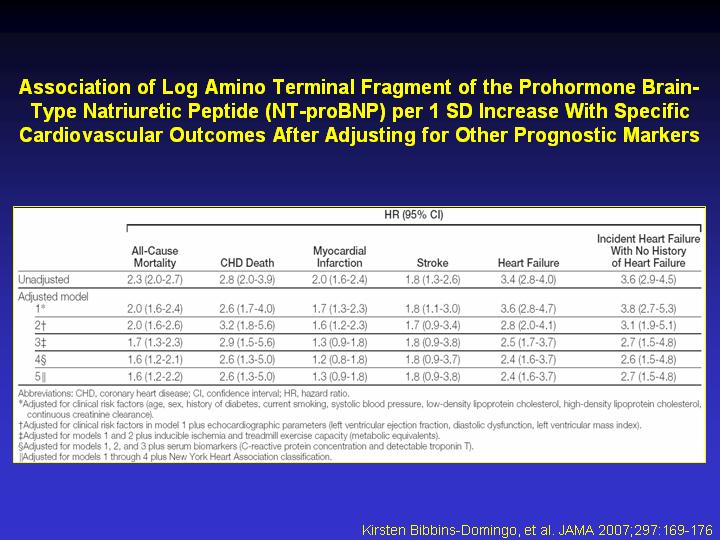
CONTEXT: Identification of individuals at high risk for cardiovascular events is important for the optimal use of primary and secondary prevention measures. OBJECTIVE: To determine whether plasma levels of amino terminal fragment of the prohormone brain-type natriuretic peptide (NT-proBNP) predict cardiovascular events or death independent of other available prognostic tests. DESIGN, SETTING, AND PARTICIPANTS: Prospective cohort study (2000-2002) of 987 individuals in California with stable coronary heart disease in the Heart and Soul Study, who were followed up for a mean of 3.7 (range, 0.1-5.3) years. MAIN OUTCOME MEASURES: The association of baseline NT-proBNP levels with death or cardiovascular events (myocardial infarction, stroke, or heart failure). Traditional clinical risk factors, echocardiographic measures, ischemia, other biomarkers, and New York Heart Association classification were adjusted for to determine whether NT-proBNP levels were independent of other prognostic factors. Receiver operating characteristic (ROC) curves were used to assess the incremental prognostic value of adding NT-proBNP level to these other measures. RESULTS: A total of 256 participants (26.2%) had a cardiovascular event or died. Each increasing quartile of NT-proBNP level (range of quartile 1, 8.06-73.95 pg/mL; quartile 2, 74-174.5 pg/mL; quartile 3, 175.1-459 pg/mL; quartile 4, > or =460 pg/mL) was associated with a greater risk of cardiovascular events or death, ranging from 23 of 247 (annual event rate, 2.6%) in the lowest quartile to 134 of 246 (annual event rate, 19.6%) in the highest quartile (unadjusted hazard ratio [HR] for quartile 4 vs quartile 1, 7.8; 95% confidence interval [CI], 5.0-12.1; P<.001). Each SD increase in log NT-proBNP level (1.3 pg/mL) was associated with a 2.3-fold increased rate of adverse cardiovascular outcomes (unadjusted HR, 2.3; 95% CI, 2.0-2.6; P<.001), and this association persisted after adjustment for all of the other prognostic measures (adjusted HR, 1.7; 95% CI, 1.3-2.2; P<.001). The addition of NT-proBNP level to standard clinical assessment and complete echocardiographic parameters significantly improved the area under the ROC curves for predicting subsequent adverse cardiovascular outcomes (0.80 for clinical risk factors and echocardiographic parameters plus log NT-proBNP vs 0.76 for clinical risk factors and echocardiographic parameters only; P = .006). CONCLUSIONS: Elevated levels of NT-proBNP predict cardiovascular morbidity and mortality, independent of other prognostic markers, and identify at-risk individuals even in the absence of systolic or diastolic dysfunction by echocardiography. Level of NT-proBNP may help guide risk stratification of high-risk individuals, such as those with coronary heart disease.
|
|