| Authors |
Schramm TK, Gislason GH, Køber L, Rasmussen S, Rasmussen JN, Abildstrøm SZ, Hansen ML, Folke F, Buch P, Madsen M, Vaag A, Torp-Pedersen C. |
|
| Title |
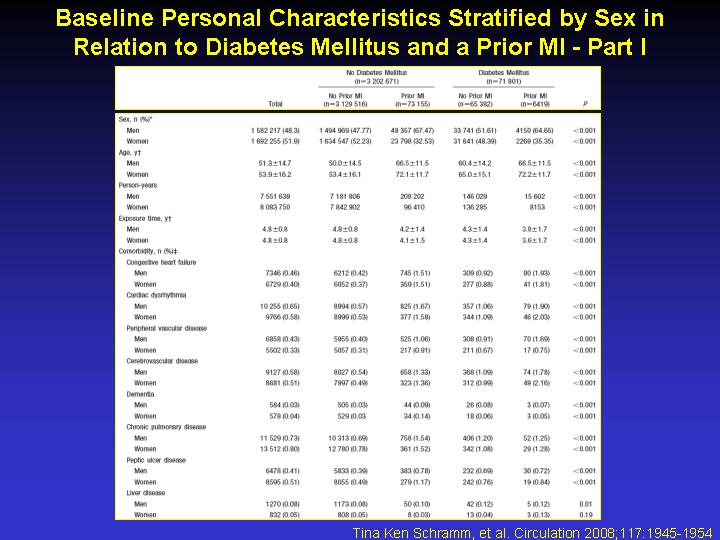
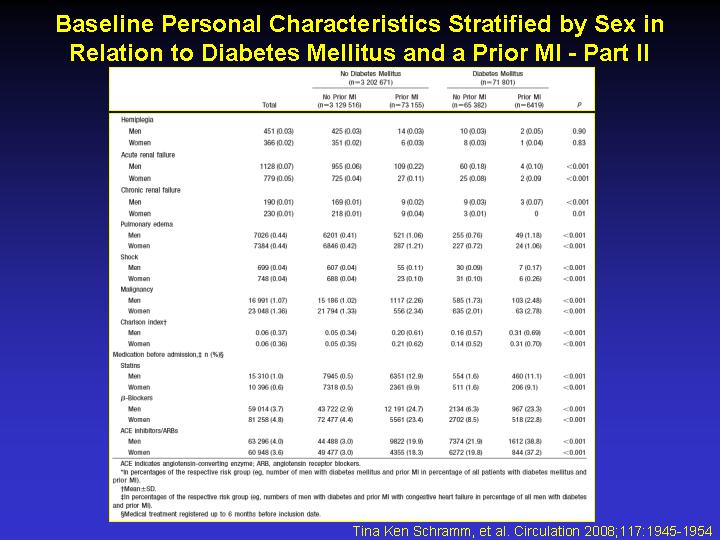
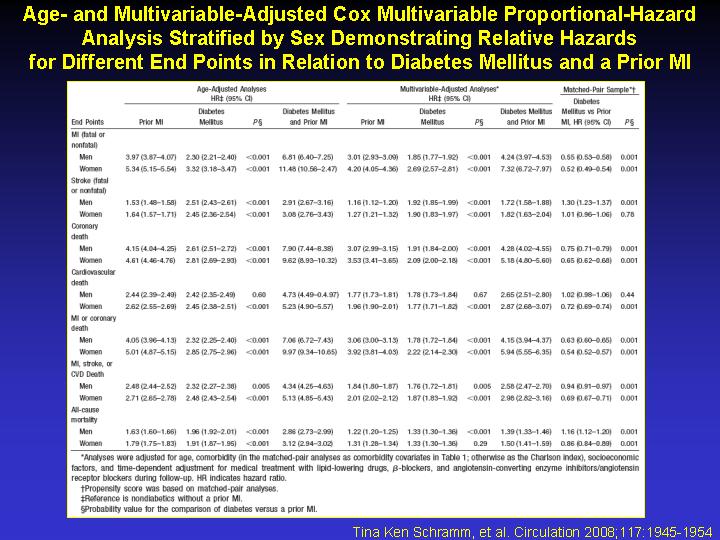
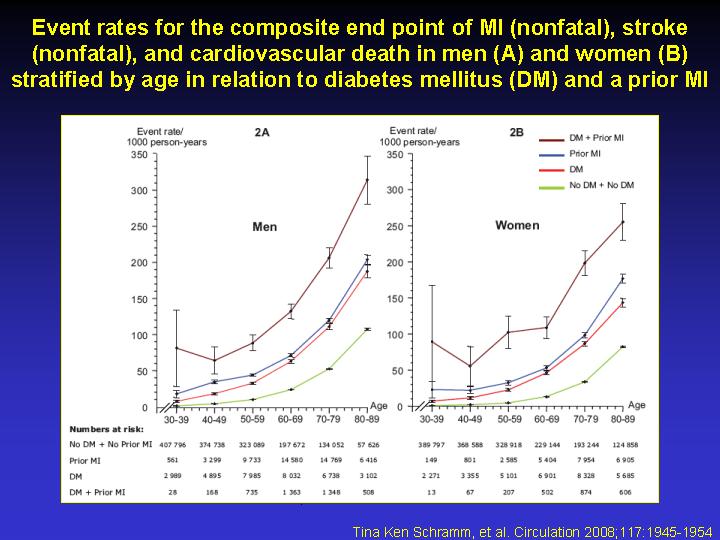
Diabetes patients requiring glucose-lowering therapy and nondiabetics with a prior myocardial infarction carry the same cardiovascular risk: a population study of 3.3 million people |
|
| Full source | Circulation 2008;117:1945-54 | |
|
|
Per scorrere le diapositive |
|
|
||
| Abstract |
BACKGROUND: Previous studies reveal major differences in the estimated cardiovascular risk in diabetes mellitus, including uncertainty about the risk in young patients. Therefore, large studies of well-defined populations are needed. METHODS AND RESULTS: All residents in Denmark > or = 30 years of age were followed up for 5 years (1997 to 2002) by individual-level linkage of nationwide registers. Diabetes patients receiving glucose-lowering medications and nondiabetics with and without a prior myocardial infarction were compared. At baseline, 71 801 (2.2%) had diabetes mellitus and 79 575 (2.4%) had a prior myocardial infarction. Regardless of age, age-adjusted Cox proportional-hazard ratios for cardiovascular death were 2.42 (95% confidence interval [CI], 2.35 to 2.49) in men with diabetes mellitus without a prior myocardial infarction and 2.44 (95% CI, 2.39 to 2.49) in nondiabetic men with a prior myocardial infarction (P=0.60), with nondiabetics without a prior myocardial infarction as the reference. Results for women were 2.45 (95% CI, 2.38 to 2.51) and 2.62 (95% CI, 2.55 to 2.69) (P=0.001), respectively. For the composite of myocardial infarction, stroke, and cardiovascular death, the hazard ratios in men with diabetes only were 2.32 (95% CI, 2.27 to 2.38) and 2.48 (95% CI, 2.43 to 2.54) in those with a prior myocardial infarction only (P=0.001). Results for women were 2.48 (95% CI, 2.43 to 2.54) and 2.71 (95% CI, 2.65 to 2.78) (P=0.001), respectively. Risks were similar for both diabetes types. Analyses with adjustments for comorbidity, socioeconomic status, and prophylactic medical treatment showed similar results, and propensity score-based matched-pair analyses supported these findings. CONCLUSIONS: Patients requiring glucose-lowering therapy who were > or = 30 years of age exhibited a cardiovascular risk comparable to nondiabetics with a prior myocardial infarction, regardless of sex and diabetes type. Therefore, requirement for glucose-lowering therapy should prompt intensive prophylactic treatment for cardiovascular diseases.
|
|